Is Eyelid Filler the Right Solution for Your Sunken Eyes? Clinical Considerations for Upper Eyelid Volume Restoration in Cheongdam-dong
Why Do Upper Eyelids Lose Volume and Look Sunken Over Time?
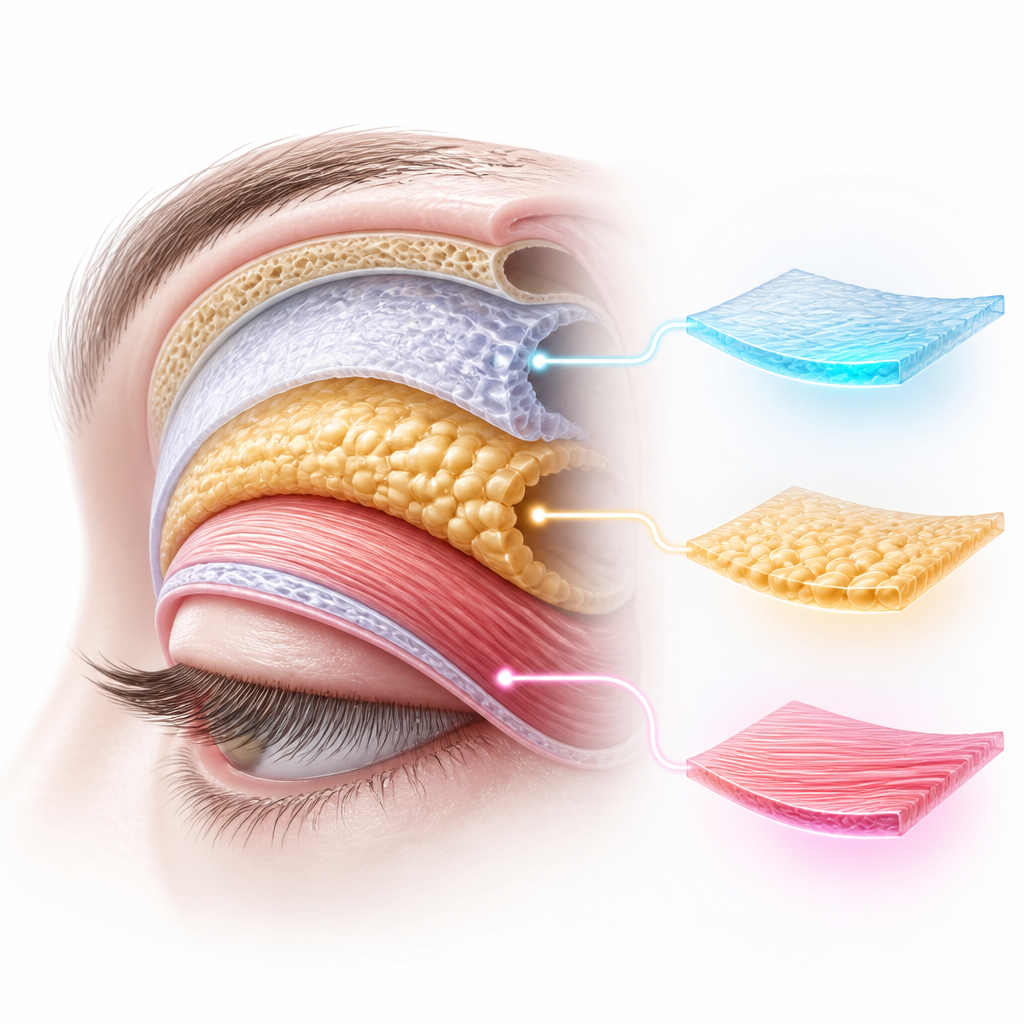
The upper eyelid area is one of the most structurally complex and delicate regions of the human face. A hollow upper eyelid, clinically referred to as superior sulcus depression, is characterized by a progressive resorption of orbital fat pads, thinning of the overlying dermis, and a gradual loss of elasticity in the orbital septum. This condition is inherently progressive; as we age, the structural support of the eye diminishes, leading to a deep hollow or ‘sunken’ appearance. The constant movement of the levator palpebrae superioris muscle—the main muscle responsible for lifting the eyelid—further accelerates the displacement and atrophy of the preaponeurotic fat pad. For individuals seeking rejuvenation in Cheongdam-dong, understanding this underlying pathophysiological mechanism is crucial before undergoing any corrective procedure.
Treatment timing: Intervention is indicated when the superior sulcus depression causes functional eye fatigue, friction during blinking, or visible aesthetic distress that does not respond to topical hydration.
Non-surgical care: Conservative management, such as topical skin-barrier repair and microcurrent stimulation, is reasonable for early-stage hollowing (Grade 1 sulcus depression) where structural fat atrophy has not yet compromised the eyelid’s natural fold.
Treatment selection: The choice between dermal filler and alternative options depends on the depth of the hollow, the patient’s orbital anatomy, skin laxity, and the presence of underlying blepharoptosis.
What Are the Non-Surgical and Conservative Management Options for Early-Stage Upper Eyelid Hollowing?
Before proceeding with injectable treatments, patients often explore conservative management strategies. For early-stage hollowing, non-surgical alternatives aim to optimize the skin’s dermal density and support the surrounding tissue. These methods include the application of medical-grade topical formulations containing peptides and retinoids to stimulate local collagen synthesis, the use of microcurrent therapy to tone the orbicularis oculi muscle, and lifestyle adjustments to reduce chronic inflammation and eye strain. However, while these strategies can improve superficial skin texture and elasticity, they cannot physically replace lost deep fat volume. Conservative care remains highly reasonable and recommended for patients with minimal structural deficit who do not yet exhibit significant shadow casting or friction-induced blinking fatigue.
How Does Hyaluronic Acid Filler Compare to Autologous Fat Grafting for Upper Eyelid Restoration?
When conservative methods are no longer sufficient, medical intervention becomes necessary. The two primary modalities for restoring volume to the superior sulcus are hyaluronic acid fillers and autologous fat grafting. Each approach presents distinct clinical profiles, and selecting the appropriate method requires careful evaluation of their respective benefits and limitations. According to multiple observational studies and meta-analyses, including a comprehensive review in the Archives of Aesthetic Plastic Surgery (2022), hyaluronic acid fillers offer immediate, reversible, and highly controllable volume adjustment, whereas autologous fat grafting provides a more permanent but less predictable long-term survival rate of the transferred fat cells.
| Parameter | Hyaluronic Acid Eyelid Filler | Autologous Fat Grafting |
|---|---|---|
| Primary Advantage | High reversibility using hyaluronidase; precise volume titration during the procedure. | Autologous material with long-term biocompatibility and potential permanence. |
| Primary Limitation | Temporary duration (typically 12 to 18 months), requiring periodic touch-ups. | Risk of irregular fat survival (lumpiness) that is highly difficult to correct without surgery. |
| Recovery Time | Minimal downtime (1 to 3 days for minor swelling). | Moderate downtime (1 to 2 weeks for swelling and bruising at donor and recipient sites). |
According to official guidelines or academic evidence, both quantitative criteria and clinical judgment should be reviewed together. In the delicate upper eyelid region, safety profiles and reversibility often serve as the primary clinical decision-making factors.
What Are the Quantitative Selection Criteria and Potential Risks of Upper Eyelid Filler?
Safety is the paramount consideration when treating the periorbital region due to the complex vascular network branching from the ophthalmic artery. Clinicians in Cheongdam-dong must adhere to strict protocols to minimize the risk of complications such as vascular occlusion, bruising, or the Tyndall effect (a bluish discoloration caused by superficial placement of filler). According to domestic and international clinical guidelines, utilizing a blunt-tip micro-cannula (typically 27G or 25G) is highly recommended over sharp needles to reduce the probability of vessel penetration. Furthermore, volume should be introduced slowly and in micro-droplets, rarely exceeding 0.3cc to 0.5cc per eyelid in a single session.
However, outcomes may differ in exceptional cases such as patients who have previously undergone upper blepharoplasty, which can alter the normal anatomical tissue planes and create dense scar tissue, or patients with underlying severe aponeurotic ptosis who require surgical muscle repair rather than volume replacement.
To determine if you are a candidate for upper eyelid filler, review the following clinical indicators:
- Moderate to severe superior sulcus depression (Grade 2 or 3) causing a tired or aged appearance.
- Good skin elasticity of the upper eyelid without excessive sagging (dermatochalasis).
- Absence of severe true ptosis (drooping eyelids caused by levator muscle weakness).
- Realistic expectations regarding the temporary nature of hyaluronic acid fillers.
- No history of hypersensitivity to hyaluronic acid or local anesthetics.
Below is a quick decision-making mini-flow to guide your initial assessment:
- Step 1: Evaluate if the hollowing is accompanied by severe skin laxity. If yes, consider surgical blepharoplasty; if no, proceed to Step 2.
- Step 2: Check for levator muscle function. If true ptosis is present, prioritize ptosis correction surgery; if ptosis is absent, proceed to Step 3.
- Step 3: Select hyaluronic acid filler with a blunt cannula for immediate, safe, and reversible restoration of the hollow upper eyelid.
Frequently Asked Questions FAQ
QIs the procedure for upper eyelid filler safe given the proximity to the eye?
Yes, when performed by an experienced specialist using a blunt micro-cannula, the procedure is highly controlled. By placing the filler deep beneath the orbicularis oculi muscle and avoiding sharp needle injections, the risk of vascular injury is minimized.
QHow long does hyaluronic acid filler in the upper eyelid typically last?
Due to the relatively low mobility of the upper eyelid compared to other facial areas, hyaluronic acid fillers in this region tend to last longer, often between 12 to 18 months. However, individual metabolic rates and tissue characteristics can influence the longevity.
QCan upper eyelid filler correct a double eyelid fold that has become multiple folds?
Yes, when loss of volume causes the eyelid skin to drape unevenly and create multiple shallow folds, restoring volume with filler can smooth the surface and help re-establish a single, clean double eyelid crease.

This content is general medical information, and individual treatment decisions should be made through imaging tests and in-person medical evaluation.
Author: Medical content editor based on medical information research
Reviewed by: Specialist consultation from the relevant department
Last reviewed: 2026-06-22
Reference guideline: 2023 International Society of Aesthetic Plastic Surgery (ISAPS) Patient Safety Guidelines
Medical neutrality and closing note
The core of medical decision-making is not to follow a specific device or a trending procedure, but to choose an option that fits each patient’s individual anatomy, condition, risk level, and treatment goals. Every procedure has both advantages and limitations, so decisions should be made after sufficient discussion with an experienced specialist.
[Medical information and copyright notice]
This content is a professional medical column prepared based on medical consultation from 청담큐비큐의원.
The infographics used in this article are created to support understanding and may differ from actual clinical results.
The information provided is a general medical guideline, and accurate diagnosis and treatment require an in-person evaluation by a qualified specialist.